







Endometriosis
Endometriosis is a common gynecological condition. It is a condition in which the cells that line the uterus grow outside of the uterus in other areas such as the ovaries. It is a chronic, painful, and often progressive disease in women. It also interferes with a woman’s fertility and ability to become pregnant. The cause of endometriosis is unknown and it is widely variable in symptoms and severity and it is difficult to diagnose.
Endometriosis occurs when cells from the mucus membrane lining the uterus (endometrial) form implants that attach, grow and function outside the uterus, generally in the pelvic region. The endometrial cells contain receptors that bind to estrogen and progesterone which promote uterine growth and thickening. When these cells become implanted in organs and structures outside the uterus these hormonal activities continue to occur causing bleeding and scarring.
Endometriosis lesions can be found anywhere in the pelvic cavity , on the ovaries, the fallopian tubes and on the pelvic side wall. In rare cases endometriosis has been found inside the vagina, inside the bladder, on the skin, lung, spine and brain.
The most common symptoms of endometriosis is pelvic pain. This pain often correlates to the menstrual cycle. It has been felt by the specialist that endometriosis is likely to be found in women who have never been pregnant. Sometimes it affects women who have had children and it can also occur in teenagers also.
Endometriosis can usually be treated by medications or surgery designed to preserve fertility. Few patients have severe symptoms of endometriosis where they have advised to undergo surgical removal of uterus and ovaries. But for most of the patients alternative treatment are available and hysterectomy is rarely necessary.
THE FEMALE REPRODUCTIVE ORGANS
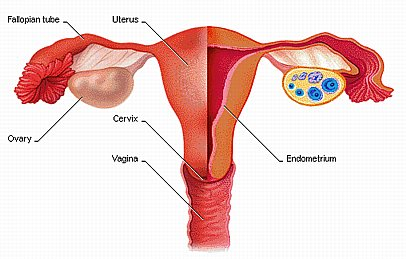
A basic knowledge of these organs and their functions is essential to understand endometriosis. The female reproductive system or genitalia has two main parts, namely the uterus and the ovaries. The uterus is a hollow organ in the center of the pevis with pear shape. The uterus houses the fetus during its development stage. It also produces secretions in the vagina and the uterus as well. On the other hand the ovaries produces the egg cells. The two fallopian tubes are attached to the upper part of the uterus to the ovaries one on each side. During periods the ovaries release an ovum through the fallopian tube. When during such release the sperm meets the ovum, fertilization occurs. In fertilization the sperm and egg meet most commonly in the oviducts or the fallopian tube. This process may occur within the uterus. Then the fertilized egg implanted in the walls of the uterus to commence further changes or processes such as embryogenesis. After a period of nine months, when the embryo is well developed in order to survive apart from the womb, the cervix dilates and contractions occurs in the uterus which pushes the fetus through the vagina which is commonly known as child birth.
However if fertilization does not occur the ova is released approximately every month a process commonly known as menstruation.

CAUSES OF ENDOMETRIOSIS
Hormone level affect the course of endometriosis and are related to the menstrual cycle. Endometriosis is less severe when the hormone levels are more constant
Several theories may explain how endometriosis develops as follows:
One popular theory focuses on a potential process known as retrograde menstruation. Retrograde menstruation is backward flow during a period. Where the menstrual products, including endometrial cells, may escape into the body through the Fallopian tubes and are deposited onto internal structures such as the ovaries, the bladder, and portions of the large intestine. These endometrial cells implant on the ovaries or elsewhere in the pelvic cavity and have a increased chance of developing endometriosis. However retrograde menstruation alone is not the cause of endometriosis since it has been shown to occur commonly in many women. Other causative factors may play roles in determining which women develop endometriosis.
Transfer of endometrial tissues by a surgical procedure might be the cause for endometriosis implants seen in surgical scars (e.g) episiotomy or cesarean section
Another possible explanation for the cause of endometriosis includes immune response in women with endometriosis. Abnormalities in the immune system may play a vital role in the development of the condition
The rare cases of endometriosis that develop in the brain or other distant organs are likely due to the spread of endometrial cells via the bloodstream or lymphatic system.
Genetic factors are also involved for the cause of endometriosis. Women who have sisters or a mother with endometriosis have a greater chance of the disease. The reason why some women develope endometriosis while others do not have is not completely explained.
SYMPTOMS OF ENDOMETRIOSIS
- Pain before and during periods
- Pain with intercourse
- General, chronic pelvic pain throughout the month
- Low back pain
- Heavy and/or irregular periods
- Painful bowel movements, especially during menstruation
- Painful urination during menstruation
- Fatigue
- Infertility
- Diarrhoea or constipation
Other symptoms which are common with Endometriosis include:
- Headaches
- Low grade fevers
- Depression
- Hypoglycaemia (low blood sugar)
- Anxiety
- Susceptibility to infections, allergies

DIAGNOSIS
Endometriosis can be suspected based on symptoms of pelvic pain, fertility problems, severe menstrual cramps or pain during intercourse. Physical examination of the pelvic by your doctor is one way of finding the presence of endometriosis. The rectovaginal examination (one finger in the vagina and one finger in the rectum) the doctor can feel nodules behind the uterus and along the ligaments that attach to the pelvic wall. But the examination itself causes unusual pain or discomfort. Pelvic examination cannot confirm the presence of endometriosis.
ULTRASOUND: Imaging studies such as ultrasound will be helpful in ruling out other pelvic diseases and may suggest the presence of endometriosis in the vaginal and bladder areas. For an accurate diagnosis, direct visual inspection inside the pelvis and abdomen as well as tissue biopsy of the implant is necessary. In special cases, computerized tomography(CT Scan), or magnetic resonance imaging (MRI) to get more information about the extent of endometriosis.
The only accurate way of diagnosing endometriosis at the time of surgery either by open
Surgery with large incision or laparoscopic surgery with small incision.
Laparoscopy is the most common surgical procedure for the diagnosis of endometriosis. It is a minor surgical procedure done under general anesthesia or local anesthesia for some cases it is performed as a outpatient procedure. Laparoscopy is a thin lighted telescope is inserted into the abdominal cavity through a small incision in or near the navel. Looking through the laparoscope the surgeon can inspect the abdomen, pelvis and the endometrial implants can be directly seen. Laparoscopy will provide information about the location and size of implants, information to be used in choosing treatment. Some times the signs and symptoms are so obvious that laparoscopy may not be necessary. During laparoscopy a small piece of tissue can be removed for microscopic examination which is called as biopsy.
Blood tests for endometriosis (CA125)
It has been indicated by the recent studies that women with endometriosis have elevated level CA125 in blood. This is tumor marker most commonly used to diagnose ovarian cancer. It has been found that 30-60% of all cases of endometriosis can have increased level of this blood test. Not all women who have endometriosis have a positive CA125 test, especially those women with mild disease. This test is not specific to endometriosis, it can be positive in a number of other diseases such as fibroids, infections, recent surgery and cancer.
Treatment
There is no known cure for endometriosis. But , there are treatments which can help to relieve your symptoms and improve your quality of life. To find our the right solution for your problem, you should talk with your doctor about your symptoms, how they affect your daily life, and discuss whether you want to have children now or in the future.
Hormonal treatments
The goal of hormonal treatment is to stimulate pregnancy or menopause, two natural conditions known to inhibit the disease. We know the cause of endometriosis remains unknown but, we know the disease is exacerbated by oestrogen. Therefore hormonal treatments for endometriosis are designed to attempt to temper oestrogen production in a woman’s body. These hormonal therapy is used to suppress the menstrual period to prevent the monthly bleeding
There are several types of medications that act by shrinking the lining of the uterus and the endometriosis lesion.
The oral contraceptive pill - The pill is one of the most commonly used treatments for endometriosis and is a good choice for young women with mild disease who also require effective contraception. It is compared with GnRH agonists and found an equal improvement with both drugs with regards to pelvic pain, painful periods, and painful sex. Many gynecologists suggest that it is better taken continuously and it does not do any harm to your body. It contains one of the hormones that keeps the lining of the womb quite thin. If used continuously, it should be for 6-12 months, but breakthrough spotting is common.
Progestines/progesterone – Progestogens are the most commonly used medical treatment and are effective in about 80% of cases. This can prescribes as pills or injections. They work by thinning out and shrinking down the endometriosis and also by suppressing the normal cycle of the ovary. They can be used either continuously or in a cyclical way ( taken for 3 weeks with one week off). Side effects of progestogens include irregular vaginal bleeding ,water retention, weight gain. They are less expensive than the other medications.
GnRH-Analogues- It stands for Gonadotrophin releasing hormone and an agonist is a drug that acts the same way as the body’s own hormone. The body normally makes GnRH in the same gland in the brain (pituitary gland) and it stimulates the ovary to develop eggs and produce oestrogen leading to the normal menstrual cycle. When the analog treatment was started, it leads to the depletion of pituitary hormones which direct the ovary to release estrogen. It effectively makes you menopausal for the short time that you use the treatment cycle and without the estrogen stimulation, endometriosis shrinks down and becomes inactive. The side effects of this treatment is hot flushes, reduced sex drive, vaginal dryness, emotional symptoms, depression and headaches.
Danazol- Danazol is a hormone derivative used to treat endometiosis. It works by preventing ovulation and reducing oestrogen levels as well as having a directly suppressive effect on the endometriosis. It has some properties that are similar to the male hormones testosterone and may have side effects like weight gain, water retention, tiredness, decreased breast size. Danazol controls pain tn the majority of patients will less extensive endometriosis and may eliminate small patches of the disease. Unfortunatley, large ovarian endometriomas (cysts) are generally resistant to the drug.
Laparoscopy Management For The Treatment For Endometriosis
Usually, if minimal to moderate endometriosis is found, a diagnostic laparoscopy will be combined with an operative laparoscopy. An operative laparoscopy procedure is performed to remove any endometriosis lesions and adhesions surgically. That is any endometriosis are diagnosed and treated at the same time and only one operation is needed.
The surgical procedures that may be performed during an operative laparoscopy include:
- removal or destruction of endometrial implants
- removal or destruction of ovarian endometriosis (endometriomas)
- removal of adhesions
- removal of deep rectovaginal and rectosigmoid endometriosis
- removal of the uterus (hysterectomy)
- removal of one or both ovaries
- surgery of the bowel or bladder
- laparoscopic uterine nerve ablation (LUNA) and presacral neurectomy (PSN).
The laparoscope is like a miniature telescope with a lenses for a clear view, that is inserted through the small incision just below the navel. A special attachment transmits light down through the tube into the abdomen, so that the surgeon can see the ovaries, fallopian tubes and near by organs. Once the procedure is completed the instruments are removed and the wound is closed.
For the patients who have no success with any treatment and who have completed their families, the ovaries may be removed to relieve severe and persisting pain. The uterus is also removed at this time. This may reduces the chance of recurrence but, this leaves a woman in a estrogen - deficient state. In such case subsequent estrogen replacement therapy is needed.
Treatment of infertility associated with endometriosis
Endometriosis is very common in infertile, compared to fertile women. It does not fully prevent conception of a women with endometriosis, they still be able to conceive especially those with mild to moderate endometriosis. The endometriosis involves masses of tissue or scarring within the pelvis that may distort normal anatomical structures such as fallopian tube which transport the egg from the ovaries. Endometriosis may affect fertility through the production of hormones and other substances that have a negative effect on ovulation, fertilization of egg or implantation of embryo.
Treatment for infertility is associated with endometriosis are varied but, when the goal is for the enhancement of fertility surgical treatment are superior to hormonal or medical treatments for endometriosis. Assisted reproduction techniques may also be used when appropriate in combination with surgical therapy.
Endometriosis and Psychological effects
Endometriosis is associated with psychological issues in the chronic condition particularly those related to pain.. Other factors of psychosocial importance are ability to work, involvement in leisure activities, relationships and self –image. In addition, the hormonal treatments for endometriosis can affect sexuality and be emotionally difficult. The side effects of these medications, some of which mimic menopause can cause depression and inhibit sexual desire in some women. Women who experience chronic pelvic pain may well be negative effects such as anxiety, depression which in turn can impact adversely on marital and family functioning. The understanding and support of partner, family and friends are important to any woman with endometriosis.



